Case Study
(The discussed case is purely theoretical and aims to demonstrate how to deal with a client with specific ailments).
COPD/Hypertension – EXAMPLE
1. Summary of the client details
Ref PP20
Name: V. Heyward
Age: 47
BMI: 28
RHR: 75
Predicted VO2max 28ml/kg/min
Current fitness level: 8 Mets (Low)
Present physical activity level: Sedentary
Patient’s statement regarding state of change: “I would like to exercise, but I am not sure that I’ll be able to do it” (Contemplation stage of change)

2. Medical conditions
COPD: (Mild severity, caused by smoking cigarettes for 27 years)
Chronic obstructive pulmonary disease (COPD) is the name for a group of lung conditions that cause breathing difficulties.
It includes:
emphysema – damage to the air sacs in the lungs
chronic bronchitis – long-term inflammation of the airways
COPD is a common condition that mainly affects middle-aged or older adults who smoke. Many people don’t realise they have it.
The breathing problems tend to get gradually worse over time and can limit your normal activities, although treatment can help keep the condition under control.
Source: https://www.nhs.uk/conditions/chronic-obstructive-pulmonary-disease-copd/
Inclusion criteria: Mild to moderate severity at the discretion of the referring medical/health professional, preferably as part of a structured clinical intervention.
Hypertension: 126/86mmHg (medicated)
Blood pressure is recorded with 2 numbers. The systolic pressure (higher number) is the force at which your heart pumps blood around your body.
The diastolic pressure (lower number) is the resistance to the blood flow in the blood vessels. They’re both measured in millimetres of mercury (mmHg).
As a general guide:
high blood pressure is considered to be 140/90mmHg or higher
ideal blood pressure is considered to be between 90/60mmHg and 120/80mmHg
low Blood pressure is considered to be 90/60mmHg or lower
A blood pressure reading between 120/80mmHg and 140/90mmHg could mean you’re at risk of developing high blood pressure if you don’t take steps to keep your blood pressure under control.
Source: https://www.nhs.uk/conditions/high-blood-pressure-hypertension/
Inclusion criteria: Diagnosed and stable (under 180/100mmHg, prior to referral.
3. Medication

Salmeterol:
Drug group: Selective beta2 agonist (slow/long acting bronchodilators)
Reason of prescription: Salmeterol works by opening the airways making breathing easier.
Desired effect of drug: Long lasting dilation of the bronchi of the lungs for up to 12 hours.
Potential side effects: Fine tremor, nervous tension, increased HR response, tachycardia, palpitations, muscle cramps.
Possible effects during exercise: Increased HR response, tachycardia
-Tachycardia is an absolute contraindication to exercise (100bpm+ RHR). If a client has this, they will need to be referred to the medical professional.
-Increased HR response during exercise will reduce the reliability of HR training zones, so greater emphasis should be paid to alternative methods, such as RPE
Source: Wright Foundation GP Ref book page 125
Becometasone:
Drug group: Inhaled corticosteroids
Reason of prescription: Becometasone prevents inflammation in the airways making breathing easier.
Desired effect of drug: Reduced airway inflammation
Potential side effects: https://www.drugs.com/sfx/beclomethasone-side-effects.html
Possible effects during exercise: N/A
No side effects that will affect exercise prescription.
Source: Wright Foundation Exercise Ref book page 125
4. Exercise prescription framework

5. Specific/Clinical Objectives: Reasons for selection

BP down: This is the main objective of exercise referral with this condition. Hypertension can increase the risk of heart attack, stroke or kidney disease.
CHD risk down.
CV-based physical activity up: This will further improve the clients BP and health.
BF down: Lower body fat will reduce the stress put on organs by being overweight and improve self-esteem.
Improved MS conditioning: This will further improve the clients BP and health and strength which might improve confidence.
Less stress: Will improve clients wellbeing and quality of life.
Overall Kcal expenditure up: This will lower bodyfat and weight which will improve health and self-esteem.
Advice on heathy eating: This will help the client understand what they should be eating daily, which will improve health and lower BMI/BF.
Reduce smoking or stop: Improve breathing, health, BP, QoL, life expectancy and CV fitness.
Over time CR conditioning up: Improved breathing and quality of life
Improved QoL and well-being: The client will have less stress and will reduce the chance of depression or reducing symptoms of depression.
Better breathing performance and control: Better quality of life and improved fitness.
Better MSE that improves O2 uptake: Better quality of life due to better breathing and improved strength. Which will reduce or reverse frailty caused by COPD.
Improved muscle size and strength: Better quality of life due to improved strength. Which will reduce or reverse frailty caused by COPD.
Improved gait and balance (possibly): Better QoL due to less trips and falls and less anxiety and stress cause by trips and falls. Improved well-being.
6. Prospective six-week physical activity/exercise programme
Equipment (Purple)
AoDL (Blue)
Rest day (Green)
Stretches: Chest, triceps, Lats, bicep, quads, glutes, hamstring
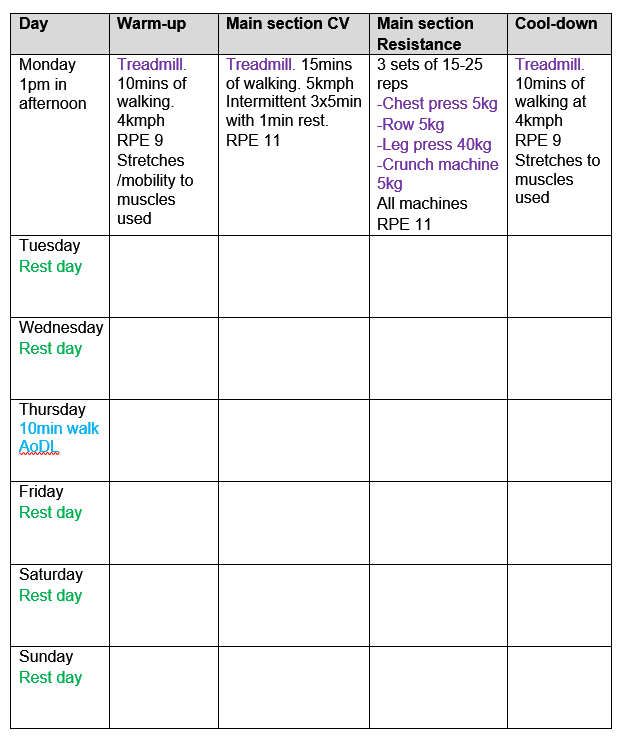
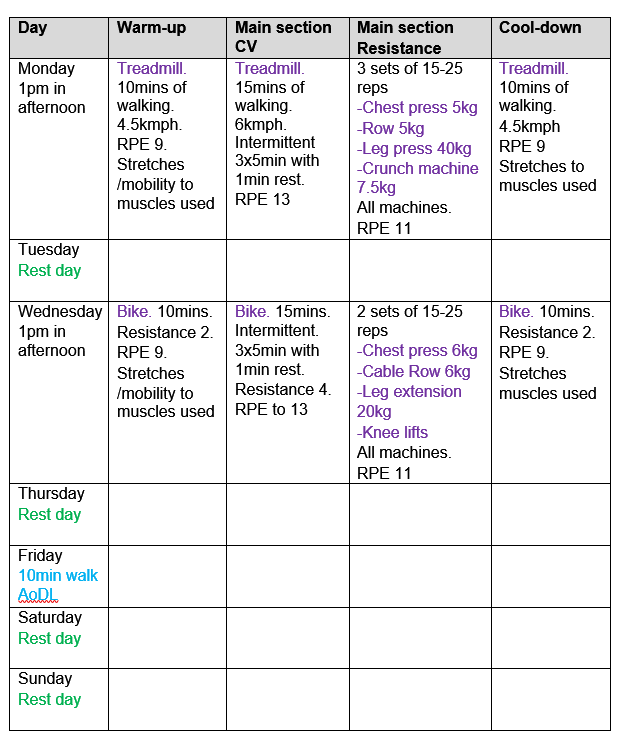
Week 1:
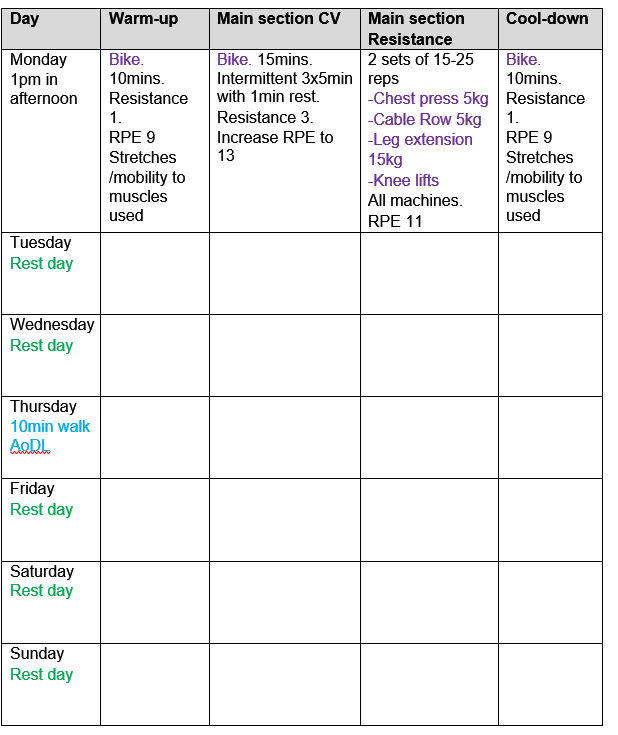
Week 2:
Week 3:
Week 4:
Week 5:
Week 6:

HRR:
HR max: 207 – (0.7×47) = 174bpm
HRR: 174 – 75 = 99bpm
Very low (0-19%):
99×0 = 99
99x.2 = 19
Low training zone:
75+0 = 75
75+19 = 94 Between 75-94bpm
Low (20-39%):
99x.2 = 20
99x.39 = 39
Low training zone:
75+20 = 95
75+39 = 114 Between 95-114bpm
Moderate (40-59%):
99x.4 = 40
99x.59 = 58
Low training zone:
75+40 = 115
75+58 = 133 Between 115-138bpm
High (60-84%):
99x.6 = 59
99x.84 = 83
High training zone:
75+59 = 134
75+83 = 158 Between 134-158bpm
METS:
28ml/kg/min divided 3.5 = 8 METS
METS training zones:
Very low = <2.4
Low = 2.4-3.7
Moderate = 3.8-5.1
High = 5.2-6.9
I will not be using high or above with this client.
7. Justification of the exercise programme
I have decided to keep all the exercise sessions structured the same with incremental increases in weight and speed. This should insure the client can get used to exercising and will also help to building confidence in the gym. After this 6 week plan I would vary the exercise sessions more to keep the client interested.
Week 1:
I have started slow with just 1 exercise session per week as client has been sedentary before being referred to me. This will give the client time get used to the new stress on their body. With a 10min walk on Thursday just to keep client more active.
Warm-up:
A thorough warm-up is required for COPD with a slow walking speed and RPE of 9 (V low). Mobility exercises to warm up and joints and stretches for the muscles/tendons.
CV:
Iv selected 15mins steady state CV exercise on the treadmill because this is will increase CV fitness without putting too much stress on client. With 1mins breaks every 5mins to allow the client to gain control of breathing again. This will be at an RPE of 11 (low). To allow for the client to get used to walking that amount of time. I am using RPE because medication can affect HR response and make HR training zones unreliable.
Resistance:
15-25 reps of 3 sets of chest press, row, leg press, crunch machine. So most of the natural movements have been used accept over head because this is a contraindication to hypertension. An emphasis on endurance and not going to MMF or using moderate to high intensity because this not safe for a client hypertension.
Cooldown:
10mins thorough cooldown is required for COPD with stretches to develop flexibility while warm after exercise.
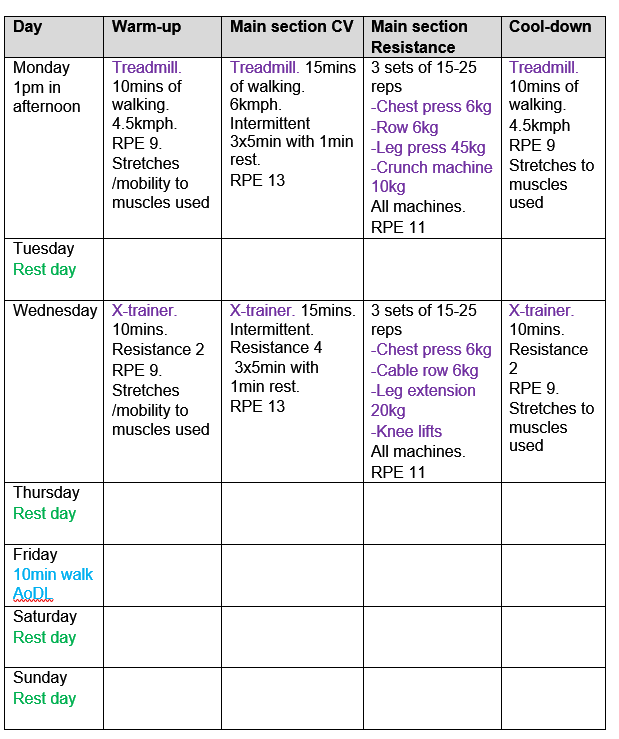
Week 2:
Still 1 session a week so the client can get used to the exercise regime and a 10min walk on Thurs. I have changed the CV and warm-up to the exercise bike. I have not changed the weight to allow the client to get used to exercise regime.
CV:
I have changed this to the exercise bike to keep the session varied. RPE has moved up to 13 (moderate).
Week 3:
2 sessions per week now the client has got used to exercising (Mon + Wed). With AoDL moved to Fri for sufficient rest (48hours).
Warm up:
Resistance and speed increased because client should be getting used to being exercise and has increased in fitness.
CV:
Resistance and speed increased to keep client at an RPE of 13 as their fitness should of increased.
Resistance:
All weights have been increased marginally on the weeks second exercise session as client should be stronger at this point of the programme (RPE 11).
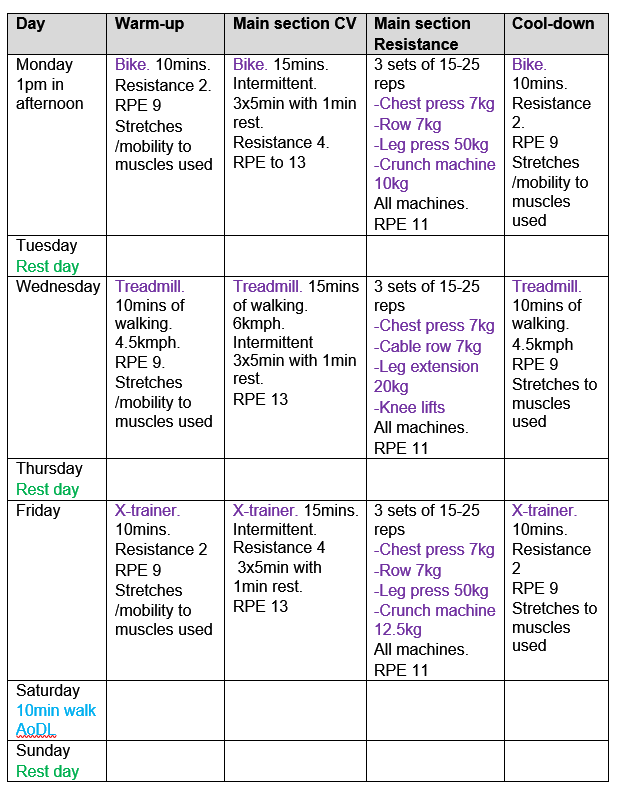
Week 4:
I have added a X-trainer into the plan now because the client fitness should be at a point to use this machine now. This also helps diversify the plan more. Everything else is the same
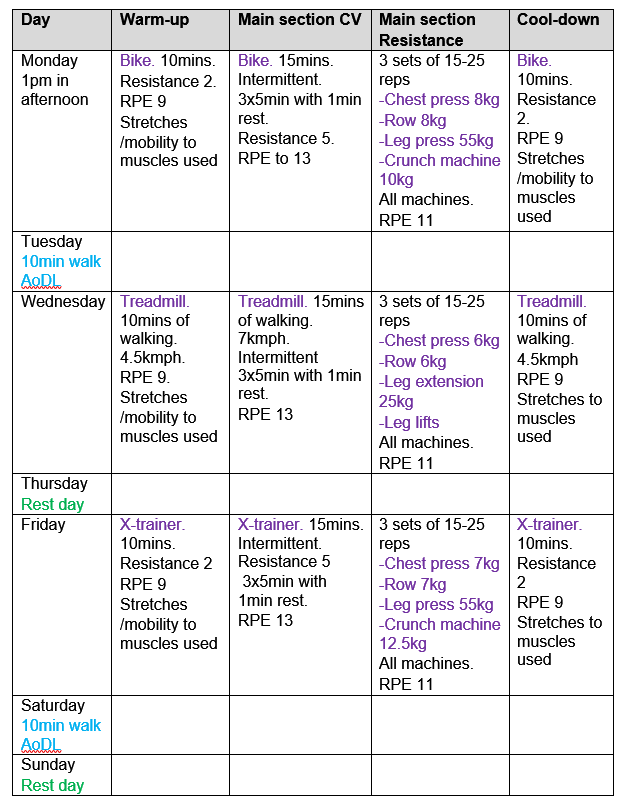
Week 5:
On week 5 I have added another exercise session because the client should be accustomed to exercising on a regular basis. 10min walk has been moved to Saturday to keep client active with rest day before the session on Monday.
CV:
This week I have put in a different CV machine each day to keep the client interested.
Resistance:
The weight of each exercise has had small increase. This is an appropriate and achievable increase in resistance as the client should be stronger.
Week 6:
Sticking with 3 sessions a week. The client should be at a point now where this is manageable. Iv added a 10min walk on Tuesday to keep the client even more active.
CV:
Another small increase in speed and resistances. This should be achievable as long as the RPE is still at 13.
Resistance:
Another small increase in weight as long as the is remains at an RPE of 11 with same rep range of 15-25. A change from knee lifts to leg lifts as the client gets stronger.

8. Psychological issues:
Stage of change and behavioural strategie
At the start I will conduct a personal interview with the client to find out what health habits they have, to what extent they are physically active, what previous experience they have with exercise and what attitude they have about changing their lifestyle.
The GP referral form shows the client has COPD and hypertension. During the interview said, “I would like to exercise, but I’m not sure if I can do it”. Which means that the client wants to exercise but is struggling with the psychological hurdle. This statement is in the contemplation stage of change according to the Transtheoretical Model.
I have decided to use a strategy that will deal with actual and perceived barriers, decision making and mechanisms for action. Fear of the unknown and failure can effectively prevent the client from achieving a healthy lifestyle. I will use the SMART goal method. The goals set will be achievable and when the client achieves these goals should see the programme as a success.
I will consistently motivate the client to continue with the programme. I will pass on knowledge of why the client is doing a particular exercise and what part of their body it’s using. This should help the client self-motivate and self-monitor in future.
I will diversify the exercise plan to reduce boredom and increase all round performance. This should help the client to have a desire to continue with the plan.
I will motivate and give the client and challenge them to actively spend their free time doing activities of daily living such as a 10min walk. This should result in additional motivation and help the client be more active in their daily life. Which should help build more confidence in self-motivation.
Based on The Social Cognitive Theory. At a late part of the programme I will try and persuade the client to join an activities group in the local community, which for example; walks, jogs, swims, etc. To give the client a support group that is active. This should strengthen and help the willingness to change habits. I will encourage the client to try new forms of activity/exercise to find one or more that makes them happy and will result in long-term maintenance of positive health.
9. Further / additional considerations
Before I start any exercise, I will check the client RHR to make sure it is under 100bpm because the client’s medication can cause tachycardia. I would also check the clients BP and make sure it’s under 180/100mmHg.
I will make sure the client is wearing suitable clothing for exercise especially footwear.
I will make sure that I take precautions while training the client with hypertension. Which are…
-Breath rhythmically
-Emphasise dynamic contractions (no isometrics)
-Use light weights (RPE-11-13, rep range 15-25)
-Use machines first
-Use light/safe grip
-Avoid gritting teeth
-Avoid MMF
-Avoid overhead movements
Source: Wright Foundation exercise referral book P176
If the client suffers from dyspnoea during any part of the exercise session I will stop and let them regain their breath and ask if they want to continue.
References:
https://www.nhs.uk/conditions/chronic-obstructive-pulmonary-disease-copd/
https://www.nhs.uk/conditions/high-blood-pressure-hypertension/
https://www.drugs.com/sfx/beclomethasone-side-effects.html
Frameworks WF exercise referral (hypertension and COPD)
WF exercise referral book
Case_study_COPD_Hypertension.pdf

